肺がんの治療法執筆者:聖路加国際病院院長 福井 次矢
肺がんとは、どんな病気でしょうか?
おもな症状と経過
(画像をクリックすると拡大)
肺がんの初期はとくに症状はなく、発生する場所にもよりますが、実際に症状が出てくるのはかなり進行してからのこともあります。肺のどの場所に発生したかで、症状やその後の経過は異なりますので、発生した場所によって肺がんを分類する方法が一般的に用いられます。
肺の入口付近にできるものを中心型肺がん(肺門部肺がん)、肺の奥のほうにできるものを末梢型肺がん(肺野部肺がん)といいます。中心型肺がんでは、比較的早い時期から、せき、痰、血痰の三大症状が現れます。かぜに似ていますが、鼻汁や頭痛、のどの痛みなどはありません。レントゲンでは見つけにくく、喀痰細胞診という痰の検査をすると、早期に見つけることができます。一方、末梢型肺がんは早期には症状がありませんが、レントゲン検査で比較的見つけやすいタイプです。
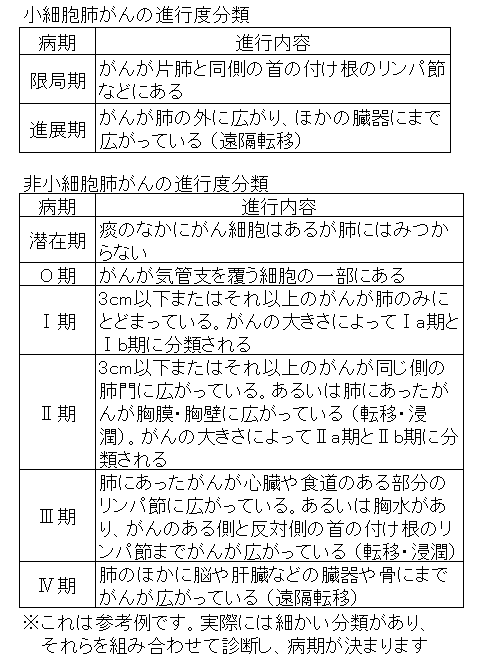
また、組織型といってがん細胞の種類による分類方法もあり、小細胞肺がんと非小細胞肺がんの二つに分類され、このうち非小細胞肺がんは腺がん、扁平上皮がん、大細胞がんに分類されます。このほか、進行の度合いによっても分類されます。一般に小細胞肺がんは進行が速く、手術ができない進行がんの状態で発見されることが多いため、予後があまりよくありません。
非小細胞肺がんは、肺がん全体の80~85パーセントを占め、その内訳は腺がん約50パーセント、扁平上皮がん約35パーセント、大細胞がん約6パーセントとなっています。治療方針はそれぞれのがんの種類によって異なります。
小細胞肺がんの病期は限局型、進展型の二つに大きく分けられ、脳や骨など体のほかの臓器にがんの転移がみられるのは進展型になります。非小細胞肺がんでは、脳やほかの臓器への転移がみられるのは進行末期のIV期になります。
病気の原因や症状がおこってくるしくみ
最大の原因はたばこで、1日の喫煙本数が多いほど、また喫煙年数が長いほど、肺がんになる確率が高くなります。それ以外では、大気汚染、慢性閉塞性肺疾患(肺気腫、慢性気管支炎)、アスベストなどの職業的暴露によって肺がんのリスクが高まると報告されています。また、肺がんの既往歴や家族歴、年齢なども肺がんのリスクを高めるといわれています。
病気の特徴
比較的お年寄りに多く発病します。現在、日本人の死因の第1位はがんですが、そのなかでも肺がんはもっとも多くなっています。病気にかかった人の数は大腸がんのほうが多いにもかかわらず、肺がんによる死亡が多いのは、それだけ治療困難な病気であることを示しています。
治療法とケアの科学的根拠を比べる
| 治療とケア | 評価 | 評価のポイント | |
|---|---|---|---|
| 予防として禁煙を励行する | ★5 | 喫煙は肺がんの原因の一つで、喫煙しない人と比べて3~5倍肺がんになりやすく、禁煙すると、喫煙を継続している人と比べて肺がんになる危険性が減少します。禁煙した期間で減少率は異なり、15年間以上禁煙した場合、喫煙者に比べて肺がんになる危険性が90パーセント減少すると報告されています。これらのことは、非常に信頼性の高い臨床研究によって確認されています。 根拠(1)~(6) | |
| 小細胞肺がん | 化学療法と放射線療法を併用する | ★5 | 小細胞肺がんは診断がついた時点で片方の肺だけに見つかることはまれで、全身のいろいろな部分に転移していることが多いので通常外科治療を行うことは少なく、行うとしても単独では行いません。化学療法、放射線療法を組み合わせた治療を行います。限局期の治療において、化学療法と放射線療法を併用した場合は、しない場合に比べて約14パーセント死亡を減少させ、3年生存率が4~7パーセント改善することが、非常に信頼性の高い臨床研究によって確認されています。ただしこの報告は全身状態のよい症例に限られており、治療前の全身状態がよくない限局期の症例では効果は明確にはされていません。一方、進展期の小細胞がんでは、全身状態の悪化が肺がんによるものであり、治療効果によって全身状態の改善が得られる可能性があれば、化学療法単独治療や放射線との併用療法により生存率を改善することが明らかにされています。 根拠(7)(8) |
| 予防的全脳照射を行う | ★5 | 小細胞がんで、初期治療で完全緩解が得られた場合には、脳転移予防のため脳全体への放射線照射(予防的全脳照射)を行うことが、信頼性の高い臨床研究で効果が確認されています。 根拠(9) | |
| 非小細胞肺がん | 早期発見、早期切除を基本に、病期(病気の進み具合)に応じた治療をする | ★5 | I~II期の治療は手術が基本になります。肺がん全体の5年生存率は35~40パーセントですが、臨床病期IA、IB、IIA、IIB期ではそれぞれ82.0パーセント、66.1パーセント、54.5パーセント、46.1パーセントという生存率が報告されています。III期で手術ができない患者さんのうち、状態がよい患者さんの場合には、放射線療法と化学療法を併用したほうが、放射線療法のみの場合よりも生存率がよくなると報告されています。IV期では、患者さんの状態がよい場合は、全身化学療法を行った場合、最良の緩和ケア(がんを治すのではなく患者さんの苦痛を取り除くためのケア)だけを行った場合に比べて、平均1.5カ月生存期間が延びたと報告されています。これらのことは、非常に信頼性の高い臨床研究によって確認されています。 根拠(10)(11)~(13)(14)~(15) |
| がん性胸膜炎には、胸水吸引後、癒着療法を行う | ★4 | 全肺がんの7~15パーセントの患者さんで経過中に悪性胸水(がん性胸膜炎の別称で、がん細胞が胸腔内にばらまいたように発生し、胸水を生じたもの)を認めます。組織型のなかでは腺がんがもっとも多いといわれています。呼吸困難がある場合には、胸水を抜きとったあとに癒着療法を行います。癒着療法は、胸水の原因となっているがんのまわりにより強い炎症をおこして癒着させ、胸水がたまる腔をなくしてしまうもので、胸腔に強い炎症をおこさせる化学物質を注入します。癒着療法の成功率は約70パーセントといわれ、副作用として痛みが平均23パーセント、発熱が平均19パーセントにおこると報告されています。こうしたことは、信頼性の高い臨床研究によって確認されています。 根拠(16)~(19) | |
| 脳転移には放射線療法を行う | ★4 | 肺がんは脳転移の頻度が高いがんです。とくに小細胞肺がんは症状があまりなく、脳に転移した状態で発見されることも多いため、患者さんの全身状態や年齢、症状を考慮し、放射線療法を行います。全脳照射が一般的で、症状の緩解が70~90パーセントの患者でみられ、対症療法として有用であるという報告があります。また、脳転移が単発である場合には、ガンマナイフなどの定位手術的照射または手術が推奨されており、全脳照射の併用は脳内再発率は下げても生存率への寄与は明確でないとされています。 根拠(20)(21) | |
| 骨転移には、放射線療法を行う | ★4 | 肺がんの骨転移は進行非小細胞肺がんでは約30~40パーセントに生じるとされます。もっとも多い症状は疼痛で、肺がんの骨転移症例の約80パーセントに認められるという報告もあります。未治療の骨転移がある非小細胞肺がんでは、可能なら全身治療としての化学療法を導入すべきです。骨転移に対する放射線治療の有効率(除痛効果)は50~80パーセントと高く、症状緩和を目的とした放射線治療はきわめて重要と考えられます。脊椎転移があり、四肢の麻痺や感覚障害などの脊髄圧迫症状がおこった場合には、緊急の放射線治療の対象になります。 根拠(22) | |
| 骨転移にゾレドロン酸またはデノスマブの投与を行う | ★4 | 骨転移のある場合は、ビスフォスフォネート(BP)製剤であるゾレドロン酸水和物や、デノスマブの投与を行うことにより、病的骨折や脊髄圧迫、高カルシウム血症などの合併症の発現率の軽減と発現までの期間を延長させることがいくつかの質の高い研究で証明されています。 根拠(23)~(26) | |
| がん化学療法に伴う好中球減少症にはG-CSF製剤を用いる | ★4 | G-CSF製剤の使用によりがん化学療法の副作用でおこる好中球減少症(白血球の一種である好中球が減少し、感染症を合併しやすくなる)による発熱は68パーセントから38パーセントへ減少したと報告されています。このことは信頼性の高い臨床研究によって確認されています。ただし死亡率を減らす効果は認められませんでした。アメリカ臨床がん学会では、慎重に使用するよう勧めています。 根拠(27)(28) | |
| 抗がん薬使用時、とくにプラチナ製剤使用時にはあらかじめ制吐薬を用いる | ★5 | プラチナ製剤を含んだがん化学療法に伴う嘔吐に対しては、5-HT3受容体拮抗薬、副腎皮質ステロイド薬、NK-1受容体拮抗薬の併用が推奨されています。 根拠(29)(30) | |
よく使われる薬の科学的根拠を比べる
抗がん薬
| 主に使われる薬 | 評価 | 評価のポイント | |
|---|---|---|---|
| ブリプラチン/ランダ(シスプラチン)+ラステット/ベプシド(エトポシド)またはトポテシン/カンプト(イリノテカン塩酸塩水和物)またはナベルビン(ビノレルビン酒石酸塩) | ★5 | プラチナ製剤のシスプラチンに、エトポシド、イリノテカン塩酸塩水和物、ビノレルビン酒石酸塩のいずれかを組み合わせた2剤併用療法の効果は、非常に信頼性の高い臨床研究で確認されています。 根拠(31)(32)(33)~(35)(36) | |
| タキソール(パクリタキセル) | ★5 | 非常に信頼性の高い臨床研究によって非小細胞肺がんに効果のあることが確認されています。 根拠(37) | |
| タキソテール(ドセタキセル水和物) | ★5 | 非小細胞肺がんのIII期またはIV期で、シスプラチンによる治療を行ったあとの患者さんに効果があったことが、非常に信頼性の高い臨床研究で確認されています。 根拠(38) | |
| パラプラチン(カルボプラチン)+ラステット/カンプト(エトポシド) | ★5 | 非小細胞肺がんのIII期またはIV期で、カルボプラチンとエトポシドを併用した場合、緩和ケアのみの患者さんと比較して効果のあったことが、非常に信頼性の高い臨床研究で確認されています。 根拠(39) | |
| ジェムザール(ゲムシタビン塩酸塩)+パラプラチン(カルボプラチン) | ★5 | ゲムシタビン塩酸塩は、カルボプラチンと併用することで非小細胞肺がんのIV期の患者さんに効果のあることが信頼性の高い臨床研究で確認されています。 根拠(40) | |
| イレッサ(ゲフィチニブ)またはタルセバ(エルロチニブ塩酸塩)またはジオトリフ(アファチニブマレイン酸)+ブリプラチン/ランダ(シスプラチン) | ★5 | 分子標的薬と言われるゲフィチニブ、エルロチニブ塩酸塩、アファチニブマレイン酸はプラチナ製剤と併用することで進行非小細胞がんの患者さんに効果のあることが、信頼性の高い臨床研究で確認されています。 根拠(41)~(46) | |
| ザーコリ(クリゾチニブ) | ★3 | ALK阻害薬と呼ばれるクリゾチニブとアレクチニブ塩酸塩は、ALK遺伝子が作り出す酵素の働きを阻害することで肺がんの増殖を止めようとする分子標的薬です。いずれの薬も、進行非小細胞がんの非扁平上皮がんという組織型でALK遺伝子に変異がある患者さんに効果があることが臨床研究で確認されています。 根拠(47)(48)(49) | |
| アレセンサ(アレクチニブ塩酸塩) | ★3 | ||
がん性胸膜炎の癒着療法に用いる薬
| 主に使われる薬 | 評価 | 評価のポイント | |
|---|---|---|---|
| ピシバニール(抗悪性腫瘍溶連菌製剤) | ★5 | ピシバニールは非常に信頼性の高い臨床研究によって効果が確認されています。2013年9月から我が国でもタルクの使用が可能になりました。 根拠(50)(51)(52) | |
| ユニタルク(タルク) | ★4 | ||
骨代謝改善薬
| 主に使われる薬 | 評価 | 評価のポイント | |
|---|---|---|---|
| ゾメタ(ゾレドロン酸水和物) | ★4 | いずれも病的骨折や脊髄圧迫、高カルシウム血症などの合併症の発現率の軽減と発現までの期間を延長させることが、いくつかの質の高い研究で証明されています。 根拠(23)~(26) | |
| ランマーク(デノスマブ) | ★4 | ||
G-CSF製剤
| 主に使われる薬 | 評価 | 評価のポイント | |
|---|---|---|---|
| ノイトロジン〔レノグラスチム(G-CSF)〕 | ★4 | レノグラスチム、フィルグラスチムともに遺伝子組み換え型G-CSFであり、いずれも好中球を増加させる効果が信頼性の高い臨床研究によって確認されています。 根拠(27)(28) | |
| グラン(フィルグラスチム) | ★4 | ||
制吐薬
| 主に使われる薬 | 評価 | 評価のポイント | |
|---|---|---|---|
| リンデロン(ベタメタゾン) | ★5 | 上記のどれかを組み合わせて使用することで、抗がん薬による吐き気がコントロールできることが信頼性の高い臨床研究によって確認されています。 根拠(29)(30) | |
| カイトリル(グラニセトロン塩酸塩) | ★5 | ||
| アロキシ(パロノセトロン塩酸塩) | ★5 | ||
| イメンド(アプレピタント) | ★5 | ||
総合的に見て現在もっとも確かな治療法
がん細胞のタイプにより治療法が異なる
肺がんは、どのような細胞のタイプなのかにより、治療方法が大きく異なります。小細胞肺がんでは、胸腔内に限局した小さい腫瘍については放射線療法と抗がん薬を組み合わせた治療を行います。胸腔内にかなり広がっている場合は全身にがん細胞が広がっている可能性が高く、抗がん薬を用います。
非小細胞肺がんでは、比較的限局している場合には手術を、そうでない場合には放射線療法や抗がん薬を組み合わせるか、またはそれぞれを単独に用いるのが一般的です。
副作用の吐き気を抑える効果的な薬剤がある
抗がん薬に伴う吐き気・嘔吐については、あらかじめ副腎皮質ステロイド薬やカイトリル(グラニセトロン塩酸塩)、アロキシ(パロノセトロン塩酸塩)、イメンド(アプレピタント)などを用いることで、かなり抑制することができます。
病態に応じた治療法がある
がんが広がったり、転移したりすることでさまざまな合併症がおきてきますので、それぞれの治療を行います。
肺がんの浸潤によるがん性胸膜炎には胸水を吸引した後、起炎薬のピシバニール(抗悪性腫瘍溶連菌製剤)やユニタルク(タルク)を使用し、癒着療法を行います。脳転移には放射線療法を、骨転移には放射線療法あるいは骨代謝改善薬のゾレドロン酸水和物やデノスマブを使用します。がん化学療法に伴う好中球減少症にはG-CSF製剤のグラン(フィルグラスチム)やノイトロジン(レノグラスチム)の使用など、それぞれの病態に有効な治療法が確立されています。
しかし、あくまでもなにもしない場合やそのほかの治療法に比べて一時的に症状を軽減できる可能性が高いことをいっているにすぎず、残念ながら、多くの患者さんでは、完全に治癒することは望めないのが現状です。
抗がん薬の再評価が進められている
近年、抗がん薬の有効性を、その副作用との兼ね合いで本当に使う価値があるかどうか、検証しようとする臨床研究が多く行われつつあります。それらの結果によっては新たな治療法が開発されたり、従来ある治療法が比較されたりして、標準的な治療法はこれからも変化していく可能性が高いと思われます。
おすすめの記事
根拠(参考文献)
- (1)加茂憲一,金子聡,吉村公雄,他.日本人におけるがん生涯リスク評価.厚生の指標.2005;52:21-6.
- (2)Wakai K, Inoue M, Mizoue T, et al. Research Group for the Development and Evaluation of Cancer Prevention Strategies in Japan. Tobacco smoking and lung cancer risk: an evaluation based on a systematic review of epidemiological evidence among the Japanese population. Jpn J Clin Oncol. 2006; 36: 309-24.
- (3)Tobacco Smoke and Involuntary Smoking. IARC Monographs, Volume 83,2004.
- (4)The Health Consequences of Smoking.A Report of the Surgeon General, 2004.
- (5)Tobacco Control: Reversal of Risk after Quitting Smoking. IARC Handbook of Cancer Prevention, Volume 11,2007.
- (6)The Health Consequences of Involuntary Exposure to Tobacco Smoke.A Report of the Surgeon General,2006.
- (7)Pignon JP, Arriagada R, Ihde DC, et al. A meta-analysis of thoracic radiotherapy for small-cell lung cancer. N Engl J Med. 1992; 327:1618-24.
- (8)Warde P, Payne D. Does thoracic irradiation improve survival and local control in limited-stage small-cell carcinoma of the lung? A meta-analysis. J Clin Oncol. 1992;10:890-5.
- (9)Aupérin A, Arriagada R, Pignon JP, et al. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. Prophylactic Cranial Irradiation Overview Collaborative Group. N Engl J Med. 1999; 341: 476-84.
- (10)Sawabata N, Miyaoka E, Asamura H, et al. Japanese lung cancer registry study of 11,663 surgical cases in 2004: demographic and prognosis changes over decade. J Thorac Oncol. 2011; 6: 1229-35.
- (11)Pritchard RS, Anthony SP. Chemotherapy plus radiotherapy compared with radiotherapy alone in the treatment of locally advanced, unresectable, non-small-cell lung cancer. A meta-analysis. Ann Intern Med. 1996;125:723-9.
- (12)Non-small Cell Lung Cancer Collaborative Group. Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. BMJ. 1995; 311: 899-909.
- (13)Marino P, Preatoni A, Cantoni A. Randomized trials of radiotherapy alone versus combined chemotherapy and radiotherapy in stages IIIa and IIIb nonsmall cell lung cancer. A meta-analysis. Cancer. 1995; 76: 593-601.
- (14)Non-Small Cell Lung Cancer Collaborative Group. Chemotherapy and supportive care versus supportive care alone for advanced non-small cell lung cancer. Cochrane Database Syst Rev. 2010; 12: CD007309.
- (15)Baggstrom MQ, Stinchcombe TE, Fried DB, et al. Third-generation chemotherapy agents in the treatment of advanced non-small cell lung cancer: a meta-analysis. J Thorac Oncol. 2007; 2: 845-53.
- (16)Tan C, Sedrakyan A, Browne J, et al. The evidence on the effectiveness of management for malignant pleural effusion: a systematic review. Eur J Cardiothorac Surg. 2006; 29: 829-38.
- (17)Dresler CM, Olak J, Herndon JE 2nd, et al. Phase III intergroup study of talc poudrage vs talc slurry sclerosis for malignant pleural effusion. Chest. 2005; 127: 909-15.
- (18)Davies HE, Mishra EK, Kahan BC, et al. Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: the TIME2 randomized controlled trial. JAMA. 2012; 307: 2383-9.
- (19)Yoshida K, Sugiura T, Takifuji N, et al. Randomized phase II trial of three intrapleural therapy regimens for the management of malignant pleural effusion in previously untreated non-small cell lung cancer: JCOG 9515. Lung Cancer. 2007; 58: 362-8.
- (20)Borgelt B, Gelber R, Kramer S, et al. The palliation of brain metastases: final results of the first two studies by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys. 1980; 6: 1-9.
- (21)Muacevic A, Wowra B, Siefert A, et al. Microsurgery plus whole brain irradiation versus Gamma Knife surgery alone for treatment of single metastases to the brain: a randomized controlled multicentre phase III trial. J Neurooncol. 2008; 87: 299-307.
- (22)Chow E, Harris K, Fan G, et al. Palliative radiotherapy trials for bone metastases: a systematic review. J Clin Oncol. 2007; 25: 1423-36.
- (23)Rosen LS, Gordon D, Kaminski M, et al. Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: a randomized, double-blind, multicenter, comparative trial. Cancer. 2003; 98: 1735-44.
- (24)Rosen LS, Gordon D, Tchekmedyian S, et al. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a phase III, double-blind, randomized trial‐the Zoledronic Acid Lung Cancer and Other Solid Tumors Study Group. J Clin Oncol. 2003; 21: 3150-7.
- (25)Henry DH, Costa L, Goldwasser F, et al. Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. J Clin Oncol. 2011; 29: 1125-32.
- (26)Vadhan-Raj S, von Moos R, Fallowfield LJ, et al. Clinical benefit in patients with metastatic bone disease: results of a phase 3 study of denosumab versus zoledronic acid. Ann Oncol. 2012; 23:3045-51.
- (27)Ozer H, Armitage JO, Bennett CL, et al. American Society of Clinical Oncology. 2000 update of recommendations for the use of hematopoietic colony-stimulating factors: evidence-based, clinical practice guidelines. American Society of Clinical Oncology Growth Factors Expert Panel. J ClinOncol. 2000;18:3558-3385.
- (28)Timmer-Bonte JN, de Boo TM, Smith HL, et al. Cost-effectiveness of adding granulocyte colony stimulating factor to primary prophylaxis with antibodies in small-cell lung cancer. J ClinOncol. 2006; 24: 2991-7.
- (29)Roila F, Herrstedt J, Aapro M, et al. Guideline update for MASCC and ESMO in the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting: results of the Perugia consensus conference. Ann Oncol. 2010; 21 (Suppl 5):v232.
- (30)Basch E, Prestrud AA, Hesketh PJ, et al. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2011; 29:4189.
- (31)Pujol JL, Carestia L, Daurès JP. Is there a case for cisplatin in the treatment of small-cell lung cancer? A meta-analysis of randomized trials of a cisplatin-containing regimen versus a regimen without this alkylating agent. Br J Cancer. 2000; 83: 8-15. (32)Amarasena IU, Walters JA, Wood-Baker R, et al. Platinum versus non-platinum chemotherapy regimens for small cell lung cancer. Cochrane Database Syst Rev. 2008;Oct 8: CD006849.
- (33)Jiang L, Yang KH, Mi DH, et al. Safety of irinotecan/cisplatin versus etoposide/cisplatin for patients with extensive-stage small-cell lung cancer: a metaanalysis. Clin Lung Cancer. 2007; 8: 497-501.
- (34)Jiang J, Liang X, Zhou X, et al. A meta-analysis of randomized controlled trials comparing irinotecan/platinum with etoposide/platinum in patients with previously untreated extensive-stage small cell lung cancer. J Thorac Oncol. 2010; 5: 867-73.
- (35)Lima JP, dos Santos LV, Sasse EC, et al. Camptothecins compared with etoposide in combination with platinum analog in extensive stage small cell lung cancer: systematic review with meta-analysis. J Thorac Oncol. 2010; 5: 1986-93.
- (36)Greco FA, Gray JR Jr, Thompson DS, et al. Vinorelbine plus cisplatin versus cisplatin plus vindesine and mitomycin C in stage IIIB-IV non-small cell lung carcinoma: a prospective randomized study. Lung Cancer. 2002;37:179-187.
- (37)Yamamoto N, Nakagawa K, Nishimura Y, et al. Phase III study comparing second- and third-generation regimens with concurrent thoracic radiotherapy in patients with unresectable stage III non-small-cell lung cancer: West Japan Thoracic Oncology Group WJTOG0105. J Clin Oncol. 2010; 28: 3739-45.
- (38)Segawa Y, Kiura K, Takigawa N, et al. Phase III trial comparing docetaxel and cisplatin combination chemotherapy with mitomycin, vindesine, and cisplatin combination chemotherapy with concurrent thoracic radiotherapy in locally advanced non-small-cell lung cancer: OLCSG 0007. J Clin Oncol. 2010; 28: 3299-306.
- (39)Helsing M, Bergman B, Thaning L, et al. Quality of life and survival in patients with advanced non-small cell lung cancer receiving supportive care plus chemotherapy with carboplatin and etoposide or supportive care only. A multicentrerandomised phase III trial. Joint Lung Cancer Study Group. Eur J Cancer. 1998;34:1036-1044.
- (40)Sederholm C, Hillerdal G, Lamberg K, et al. Phase III trial of gemcitabine plus carboplatin versus single-agent gemcitabine in the treatment of locally advanced or metastatic non-small-cell lung cancer: the Swedish Lung Cancer Study Group. J Clin Oncol. 2005; 23: 8380-8.
- (41)Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010; 11: 121-8.
- (42)Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010; 362: 2380-8.
- (43)Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL. CTONG-0802): a multicentre, open-label, randomised phase 3 study. Lancet Oncol. 2011; 12: 735-42.
- (44)Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012; 13: 239-46.
- (45)Yang JC, Schuler M, Yamamoto N, et al. LUX-Lung 3: A randomized, open-label, phase III study of afatinib versus pemetrexed and cisplatin as first-line treatment for patients with advanced adenocarcinoma of the lung harboring EGFR-activating mutations. J ClinOncol. 2012; 30 (suppl; abstr LBA7500).
- (46)Wu YL, Zhou C, Hu CP, et al. LUX-Lung 6: A randomized, open-label, phase III study of afatinib (A) versus gemcitabine/cisplatin (GC) as first-line treatment for Asian patients (pts) with EGFR mutation-positive (EGFR M1) advanced adenocarcinoma of the lung. J ClinOncol. 2013; 31 (suppl; abstr 8016).
- (47)Costa DB et al. Clinical Experience With Crizotinib in Patients With Advanced ALK-Rearranged Non-Small-Cell Lung Cancer and Brain Metastases. J ClinOncol. 2015; 33: 1881-8.
- (48)Ou SI, Ahn JS, De Petris L, et al.Alectinib in Crizotinib-Refractory ALK-Rearranged Non-Small-Cell Lung Cancer: A Phase II Global Study.J ClinOncol. 2015 Nov 23.
- (49)Sullivan I, Planchard D. ALK inhibitors in non-small cell lung cancer: the latest evidence and developments.TherAdv Med Oncol. 2016 Jan;8:32-47.
- (50)Yoshida K, Sugiura T, Takifuji N, et al. Randomized phase II trial of three intrapleural therapy regimens for the management of malignant pleural effusion in previously untreated non-small cell lung cancer: JCOG 9515. Lung Cancer. 2007; 58: 362-8.
- (51)Dresler CM, Olak J, Herndon JE 2nd, et al. Phase III intergroup study of talc poudrage vs talc slurry sclerosis for malignant pleural effusion. Chest. 2005; 127: 909-15. (II)
- (52)Davies HE, Mishra EK, Kahan BC, et al. Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: the TIME2 randomized controlled trial. JAMA. 2012; 307: 2383-9.
- 出典:EBM 正しい治療がわかる本 2003年10月26日初版発行(データ改訂 2016年1月)